Abstract
Varicose vein is the most prevalent vascular condition treated by vascular physicians. The treatment of varicose vein has transformed from predominantly open surgery to currently endovenous ablation (minimally invasive treatment).
Varicose vein
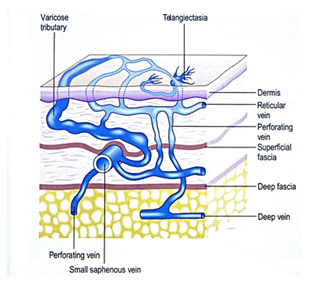
Varicose veins are prominent, dilated tortuous superficial vein usually on the legs but occasionally can be found on other parts of the body such as the lower abdominal wall and perineal area. It affects 30% of the population. The size of varicose veins varies ranging from spider vein (telangiectasia) to large bulbous varicose veins. Telangiectasias are spider veins that often have connections with the larger reticular veins and varicose veins.
Varicose vein > 3mm
Reticular vein 1-3mm
Telangiectasia < 1mm
Risk factors for varicose veins
- Older age
- Family History- A significant proportion of patients with varicose veins have other family members with varicose veins
- Female gender- Hormonal changes during puberty and pregnancy induce changes in vein wall making them more likely to dilate. The gravid uterus during pregnancy compresses on intra-abdominal major vein leading to venous hypertension in the lower extremities. Pregnancy related varicose veins usually regresses after 3-12 months
- Obesity- Obese patients have higher intra-abdominal pressure with higher venous pressure within the iliac veins and inferior vena cava. This leads to increase venous pressure in the lower extremities
- Sedentary lifestyle- The pumping action of the calf muscles is crucial in assisting venous return to the heart from the lower extremities. Patient with sedentary lifestyle often have ineffective calf muscle pump
- Occupational- People working in occupation requiring prolonged period of standing or sitting such as hairdresser, surgeon, secretary & truck driver, may suffer from varicose veins more frequently.
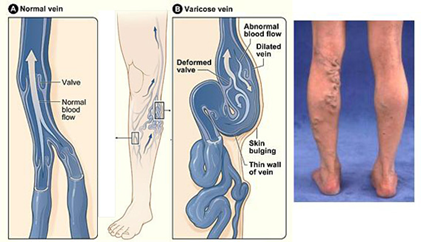
Pathophysiology
Varicose veins are due to defective functioning of the valves within the vein, allowing reflux of blood. It can cause symptoms of pain, ankle swelling, heaviness, and itchiness. Symptoms are often worse at the end of the day and after prolonged standing. More severe signs such as bleeding, brown staining of skin, eczema, and ulcer can sometime develop after many years if left untreated.
Investigations for varicose vein
Venous duplex (ultrasound) is the investigation of choice for people suffering from varicose veins.
Venous duplex provides information on
- whether the deep vein are functioning properly
- the source of varicose veins
- whether the varicose vein can be treated by minimally invasive approach
- whether there is any refluxing vein inside the abdomen contributing to the varicose veins
Arterial Doppler studies (ultrasound) may be required to assess adequacy of arterial circulation if the foot pulses are absent. Arterial disease should be treated prior to treatment of varicose vein.
Treatment
The National Institute of Health and Care Excellence (NICE) in the United Kingdom has recommended endovenous ablation as a first line treatment and those who are not suitable for endovenous therapy to be treated with surgery. Compression stocking are recommended when endovenous or surgical approach are not suitable. Australian Safety and Efficacy Register of New Interventional Procedures – Surgical (ASERNIPS) has conducted systematic review on the treatment of varicose veins and the recommendations are similar to the NICE guidelines (http://www.surgeons.org/media/300823/Varicose_Veins%28SR%29.pdf).
Endovenous thermal ablation
Endovenous treatment of varicose veins involves ablation of the refluxing great saphenous or small saphenous vein with thermal energy (radiofrequency and laser). Laser and radiofrequency ablation has been used in the treatment of refluxing vein for several years. Their results in term of recurrence of varicose veins have been found to be comparable to surgical stripping of the great saphenous vein[1]. Endovenous thermal ablation has the advantage of less pain and faster recovery to normal activities.
| Endovenous thermal ablation | Conventional surgery |
| Procedure can be performed under local anaesthesia | Procedure performed under general anaesthesia or spinal anaesthesia |
| Suitable anatomy- Non tortuous, reasonable calibre saphenous vein with no significant incompetent proximal branches close to saphenous junction | Suitable for all anatomy |
| Thermal ablation of recurrent varicose vein technically similar to primary varicose vein | Saphenous junctional ligation for recurrent varicose vein can be hazardous |
| Procedure can be performed without stopping warfarin | Anticoagulation needs to be stopped prior to surgery |
| Results equivalent or better than surgery | Surgery was the “gold standard” for varicose veins treatment previously |
| Reduced wound infection and haematoma | Wound complications more common than endovenous thermal ablation |
| Less pain and quicker return to normal activities | More painful and more prolonged recovery |
| Cutaneous nerve injury uncommon | Cutaneous nerve injury 5-10% |
| Risk of skin burn | No risk of skin burn |
| Superficial thrombophlebitis 5% | Superficial thrombophlebitis uncommon |
| Needs to combine with ambulatory phlebectomy or sclerotherapy to treat varicosities | Able to remove varicosities at the time of surgery |
Table 1: Endovenous thermal ablation versus conventional surgery
Both radiofrequency and laser endothermal ablation procedures are carried out in a similar fashion. Ultrasound is used to guide treatment. The procedure is carried out under local anaesthesia with or without sedation as day cases. The great saphenous or small saphenous vein is accessed under ultrasound guidance and a sheath is inserted into the vein. The laser or radiofrequency catheter is then passed up the refluxing vein and dilute local anaesthetic is then injected along the outside of the vein (tumescent anaesthesia). Tumescent anaesthesia provides analgesia during the procedure, and it also compresses the treated vein to prevent pooling of blood in the treated vein, thereby reducing post-operative phlebitis and increasing the success rate of occlusion of the treated vein. Tumescent anaesthesia also prevents burn injury to the surrounding tissue such as the nerve and the skin by acting as a heat sink between the treated vein and the surrounding structures. Ambulatory phlebectomy (little cut to remove the lumpy varicose veins), or sclerotherapy (injection of chemical to seal the lumpy varicose veins), can be combined with the procedure to treat the tributaries of the refluxing vein (the visible varicosities). Compression bandage is applied for 24 hours, and after removal, this is replaced by graduated compression stockings for a further two weeks. Walking is encouraged immediately after the procedure. Patient are told that phlebitis (inflammation in the treated vein) can cause pain in the treated leg after 4-5 days and over the counter non-steroidal medication (such as Nurofen or Voltaren) and Hirudoid cream applied topically are useful in the treatment of the phlebitis. In my practice, an ultrasound scan will be performed within 4 weeks, prior to post-operative clinic visit to ensure successful occlusion of the treated vein. Earlier ultrasound examination is performed if there is any suspicion of deep venous thrombosis.


Figure 1: Radiofrequency ablation of great saphenous vein
Potential complications associated with endovenous ablation
- Technical difficulties in cannulation or catheter advancement
- Deep vein thrombosis 1%
- Skin burns 1%
- Superficial thrombophlebitis 5%
- neuralgia (nerve pain) 5%
- Recurrent varicose veins 10%
Non thermal endovenous ablation
Endovenous thermal ablation of saphenous vein requires the application of tumescent anaesthesia around the saphenous vein and this requires good interventional skills and ultrasound skills. It constitutes the potentially painful part of the procedure if carried out under local anaesthesia and the most time consuming part of the procedure. Non thermal endovenous ablation does not require tumescent anaesthesia and therefore the procedure is painless and can be completed more rapidly. Non thermal endovenous ablation can complement endothermal endovenous ablation as it can be used to treat saphenous vein incompetence at the calf level with less risk of saphenous and sural nerve neuralgia (pain from nerve damage). There are two main non thermal endovenous ablation on the market currently in Australia, Clarivein and Venaseal/Venablock. Both Clarivein and Venaseal/Venablock do not receive Medicare rebate and hence patients will have to pay the full cost of the procedure.
Clarivein uses mechanical chemical means of ablating the vein. The device consist of a battery powered rotating wire that rotates at 3500rpm inside the saphenous vein, inducing endothelial (inside lining of vein) damage, and at the same time a sclerosant (chemical) such as polidocanol or sodium tetradecylsulphate was injected to enhance destruction of the vein. Results for Clarivein has been reported at greater than 90% at 2 years, however long term follow up data are not available[2]. Rotating wire can often get caught up in the wall of the vein in smaller calibre vein and often a fair amount of force is required to dislodge the catheter and this can be painful for the patient.
Venaseal/Venablock is closure of saphenous vein with cyanoacrylate adhesive. Cyanoacrylate adhesive induces an inflammatory reaction within the treated vein and causes occlusion of the treated vein. Medium term published data on the use of Venaseal in the treatment of saphenous vein reflux reported 97% occlusion rate at 12 months[3] and 94% at 3 years. The main advantage of Venaseal/Venablock is that there is no need to wear compression after the treatment.
Sclerotherapy
This treatment involves injecting sclerosing agent (chemical) into the vein to achieve sealing of the refluxing vein. It works best on the smaller calibre veins or spider vein. Sclerosant can be injected as foam or liquid. Sclerosant can be mixed with carbon dioxide gas or air to become foam (Tessari method). Foam sclerotherapy is more effective than using the liquid sclerosant directly, because the gas medium breaks up the liquid sclerosant into small bubbles and allow them to act on a greater surface area. Foam sclerotherapy however may not be suitable for the smallest spider vein, as they are too strong, and can cause significant skin staining[4]. The most commonly used sclerosants in Australia are Polidocanol (Aethoxysklerol) and Sodium Tetradecyl Sulphate (Fibrovein) which belongs to the detergent group of sclerosant. Other sclerosant that can be used includes hyperosmolar agents (e.g. hypertonic saline), and chemical irritants (glycerine and alcohol).
Potential complications of sclerotherapy
- Cutaneous pigmentation (skin staining)
- New telangiectasia (spider vein matting)
- Oedema of injected extremity
- Pain (not usually significant with polidocanol)
- Localised urticarial (rash)
- Tape blister
- Tape folliculitis (inflammation of hair follicle)
- Skin necrosis
- Systemic allergic reaction- rash, anaphylaxis
- Deep vein thrombosis
- Visual disturbance
- Stroke
- Accidental arterial injection

Figure 2: Skin staining post injection sclerotherapy

Figure 3: Telangiectasia matting after injection sclerotherapy
Skin staining is the most common adverse effect from injection sclerotherapy. Its resolution requires patience and most settled within a few months. Removal of coagulum (clot inside the vein) post sclerotherapy is an effective way of reducing skin staining in the bigger vein. Post treatment patients should avoid taking iron supplement for 1 month as serum ferritin (iron) level has been correlated with pigmentation in some studies[5]. Patients should also avoid sun exposure until treated site completely healed (use of SPF 50 sun screen recommended). Topical retinoic acid (Retin-A cream) may help speed up resolution of skin staining by enhancing fibroblast removal of hemosiderin in skin[6]. Tri-Luma cream (not readily available in Australia) consisting of a combination of Fluocinolone (mild steroid-reduce inflammation), Hydroquinone (depigmenting agent) and Tretinoin (help exfoliate skin) may also help with reducing skin staining post injection sclerotherapy.
Varicose Vein Surgery
Traditional varicose veins surgery consists of junctional ligation and stripping of the saphenous vein is still performed in Australia, however its popularity is decreasing. Result from open surgery is good with recurrence rate in the region of 10% on long term follow up. Multiple stab avulsions can be carried out at the same time. Surgery can still be a useful solution for people with multiple large varicosities that require removal at the time of surgery and those who has incompetent branches of the great saphenous vein arising very close to the saphenofemoral junction. Endovenous technology in combination with foam sclerotherapy has matured sufficiently that it can treat nearly all varicose veins without resorting to open surgery. In many cases, endovenous surgery is associated with less morbidity, especially in repeat surgery and saphenopopliteal junction (behind the knee- risk of peroneal nerve injury causing foot drop) interruption.
General advice regarding management of venous symptoms
- wear graduated compression stocking
- Graduated compression stocking counteracts the hydrostatic pressure of the varicose veins and helps reduce ankle swelling and discomfort from varicose veins.
- Regular exercise such as pedal cycling and swimming
- Exercise improves ankle movement and calf muscle pump and help reduces the hydrostatic pressure in the veins.
- Horse chestnut seed extract
- This is over the counter medication that can tone up the vein and help reduce symptoms of varicose veins.
References
- Carroll, C., et al., Clinical effectiveness and cost-effectiveness of minimally invasive techniques to manage varicose veins: a systematic review and economic evaluation. Health Technol Assess, 2013. 17(48): p. i-xvi, 1-141.
- Witte, M.E., et al., Mechanochemical Endovenous Occlusion of Varicose Veins Using the ClariVein(R) Device. Surg Technol Int, 2015. 26: p. 219-25.
- Morrison, N., et al., VeClose trial 12-month outcomes of cyanoacrylate closure versus radiofrequency ablation for incompetent great saphenous veins. J Vasc Surg Venous Lymphat Disord, 2017. 5(3): p. 321-330.
- Alos, J., et al., Efficacy and safety of sclerotherapy using polidocanol foam: a controlled clinical trial. Eur J Vasc Endovasc Surg, 2006. 31(1): p. 101-7.
- Thibault, P.K. and J. Wlodarczyk, Correlation of serum ferritin levels and postsclerotherapy pigmentation. A prospective study. J Dermatol Surg Oncol, 1994. 20(10): p. 684-6.
- Grimes, P. and J. Watson, Treating epidermal melasma with a 4% hydroquinone skin care system plus tretinoin cream 0.025%. Cutis, 2013. 91(1): p. 47-54.